110年:內專
A 54 y/o diabetic female patient with 4 days of fever, respiratory symptoms and dyspnea. At emergency service, physical examination revealed postural hypotension, tachycardia, and Kussmaul respiration. Laboratory tests were: blood glucose level of 385 mg/dL. The arterial pH is 7.35, pCO₂ is 22 mm Hg, pO₂ 86 mmHg, HCO₃⁻ 14 mEq/L. Serum electrolyte values were: Na 130 meq/L; K 5.1 meq/L; Cl 96 meq/L; Chest x-ray film indicated consolidation of bilateral lower lobe. Which of the following statements is most likely to be true? (1)The patient has respiratory acidosis, possibly related to pneumonia (2)The patient has metabolic acidosis, possibly related to diabetes (3)The patient has respiratory alkalosis, possibly related to pneumonia (4)The anion gap is still within normal range (5)Be cautious with hyperphospatemia during combined insulin and glucose therapy
A(1)+(2)+(5)。
B(1)+(2)+(4)+(5)。
C(2)+(3)+(5)。
D(2)+(3)。
E(2)+(3)+(4)。
詳細解析
本題觀念:
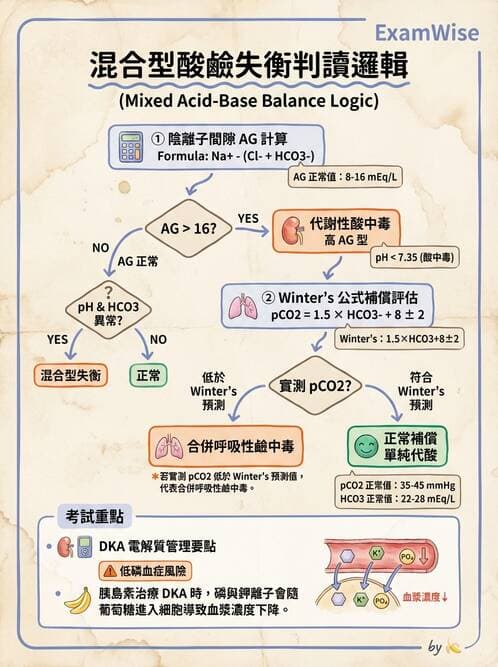
本題核心在於分析動脈血氣與電解質數值,判斷病人是否存在單純或混合型酸鹼失衡。重點包括:
- 代謝性酸中毒(metabolic acidosis)的判斷:HCO₃⁻顯著降低(14 mEq/L)。
- 呼吸性補償或另有呼吸性酸鹼異常:透過Winter’s formula預測PaCO₂,可判斷是否純代謝補償,或另有呼吸性酸中毒/鹼中毒同時存在 (en.wikipedia.org)。
- 血漿陰離子間隙(anion gap, AG)計算:AG = Na⁺ − (Cl⁻ + HCO₃⁻) = 130 − (96 + 14) = 20 mEq/L,高於正常值(約8–16 mEq/L) (emedicine.medscape.com)。
- DKA治療中電解質變化:Insulin治療常造成磷離子(phosphate)向細胞內移動,引起低磷血症 ([aafp.org](https://www.aafp.org/pubs/afp/issues/1999/0801
...(解析預覽)...
升級 VIP 解鎖圖文解析