110年:內專
Laboratory indices for differentiation of prerenal versus Intrinsic renal azotemia. Which of the followings prefers pre-renal azotemia?
AHigh urine Na concentration >20 (mmol/L)。
BHigh Urine specific gravity >1.020。
CLow urine osmolality <300 (mosmol/kg H₂O)。
DHigh renal failure index (UNa/UCr/PCr) >1。
EUrinary sediment analysis reveals a lot of muddy-brown granular casts and casts containing tubular epithelial cells。
詳細解析
本題觀念:
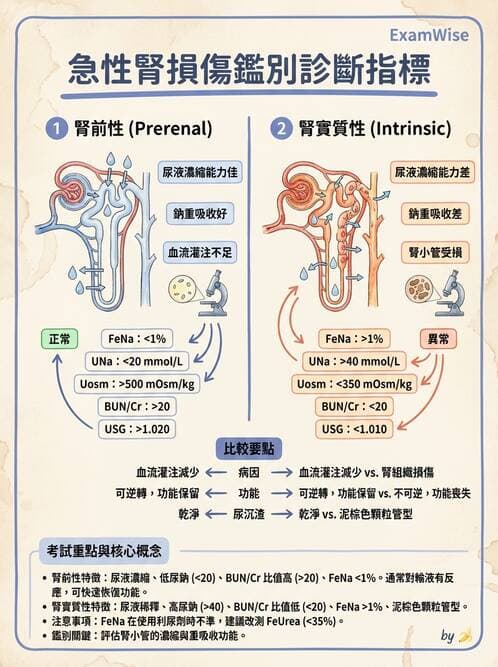
核心在於利用實驗室尿液指標區分 prerenal azotemia(前腎性氮質血症)與 intrinsic renal azotemia(腎實質性氮質血症)。前者因腎前灌注不足,腎小管功能保存完好,會表現出:
- 尿鈉濃度(UNa)低 <20 mmol/L
- 分餾排鈉率(FeNa)<1%
- 尿滲透壓(Uosm)高 >500 mOsm/kg H₂O
- 尿比重(USG)高 >1.018–1.020
- 尿沉渣僅見稀少的透明管型(hyaline casts)
intrinsic AKI(如ATN)因腎小管損傷,則相反:UNa>20、FeNa>2%、Uosm<300–350、USG<1.012、伴有泥狀褐色管型(muddy-brown casts)及管上皮細胞管型。
選項分析
-
選項A 高尿鈉濃度 >20 mmol/L
此為 intrinsic AKI(ATN)常見,prerenal 反而因水鈉重吸收增加,UNa 多低於 20 mmol/L (doctorlib.org)。 -
選項B 高尿比重 >1.020
前腎性氮質血症因腎臟保水機制活躍,使尿液濃縮,比重通常可達
...(解析預覽)...
升級 VIP 解鎖圖文解析